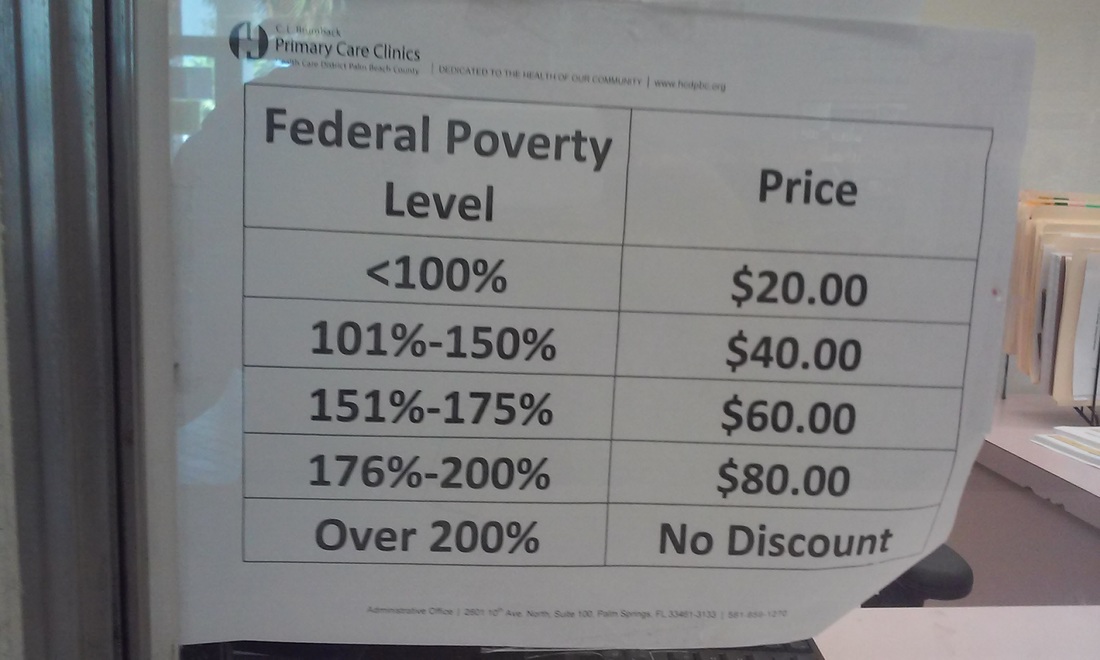
WHAT'S WRONG WITH THIS PICTURE? :: The CL Brumback Sliding Fee Schedule is very NON-Transparent. This notice posted in service windows indicates a discount (Sliding Fee Schedule), but does not disclose the 'list' cost of provider encounters, nor does it differentiate between different professional capacity levels, i.e., whether a patient is visiting an RN, an ARNP, or a Physician. From a consumer standpoint, it's problematic. Prospective patients have left the clinic without obtaining health services because they could not determine their personal liability. Additionally, this notice may be evidence of a violation of the spirit and letter of HRSA rules regarding the establishment of 'Nominal' charges. The rule states, "A nominal charge must be a fixed fee that does not reflect the true value of the service(s) provided and is considered nominal from the perspective of the patient." Nominal as defined in Google Search dictionary: "(of a price or amount of money) very small; far below the real value or cost." From the standpoint of many poor patients, $20 doesn't sound particularly 'nominal' at all, especially juxtaposed with the clinics' $36 per patient per month capitated fee for UNLIMITED primary care visits, as established by agreement between the Health Care District and the Brumback Clinics.
HRSA Policy Information Notice 2014-02:
Sliding Fee Discount and Related Billing and Collections Program Requirements:
Frequently Asked Questions (FAQs)
NOTE: New FAQs will be added as necessary. For questions regarding Outreach and Enrollment, please see the Outreach and Enrollment page: http://bphc.hrsa.gov/outreachandenrollment/index.html
PIN Section II: Applicability
1) My health center receives Section 330(h) funds. Do I have to follow the requirements of the PIN for my homeless patient population?
Yes. This PIN applies to all health centers funded under the Health Center Program authorized in section 330 of the Public Health Service Act, as amended. The PIN also applies to look-alikes, as they must meet the statutory, regulatory and policy requirements for health center program grantees under section 330. While all health centers must uniformly apply the requirements clarified in the PIN to their patient
populations, HRSA recognizes the unique challenges of serving special populations and emphasizes that a health center must consider the characteristics of its overall patient population and that population’s barriers to care when establishing and evaluating their sliding fee discount programs.
PIN Section V. Governing Board Oversight
2) Does my governing board need to develop and approve the supporting sliding fee discount program operating procedures?
No. Governing boards are required to approve the sliding fee discount program policies that establish the foundation for operating procedures. Development and implementation of related supporting operating procedures rests with the health center staff under the direction of the key management staff.
PIN Section VI: Fee Schedule
3) Are health centers permitted to have a single line on their fee schedule for a “diabetes visit” that includes the provider encounter, lab work, and a mini-session with our nutritionist?
Yes. When constructing the fee schedule, a specific health center service along with associated laboratory services and/or medically related supplies and equipment may be combined into a single fee, as long as this is consistent with both prevailing standards of care and locally prevailing charges. See Section VI.A: Fee Schedule: Services for more detail.
PIN Section VII: Sliding Fee Discount Schedule
4) Do health centers have to assess income and family size for all patients including insured patients?
Health centers must assess income and family size for all patients, both for Health Center Program reporting purposes (See UDS Reporting manual) and for determining whether they are eligible for sliding fee discounts. Eligibility for sliding fee discounts is based on income and family size and no other factors.
Health Centers May NOT Use Assets Tests as Additional Eligibility Threshold
5) Is it permissible for a health center to include assets in its definition of income?
No. Health centers may not use assets tests as an additional eligibility threshold, nor may they create a “net worth test” (i.e., a combined threshold of assets and income). Assets are not considered income; assets are an economic resource, while income is comprised of earnings over a given period of time. For example, a rental property would be considered an “asset,” but the income generated from this rental
property could be considered “income.” Health centers are permitted to request information on assets for purposes other than sliding fee discount scale eligibility, e.g., assessing eligibility for private or public benefit programs that require asset information.
6) What does a health center have to include in assessing and documenting a patient’s income?
The health center governing board determines in policy what types of income are included or excluded in defining “income,” as well as the associated documentation needed to assess income for individual patients, as long as such policies do not create barriers to care. As with all sliding fee discount program policies, the health center’s nominal charge(s) must be applied uniformly to all patients.
7) How do health centers consider family members, not living with the patient but largely supported by the patient’s income, in their definition of “family size”?
Health centers have the flexibility to define family size to include these family members as part of their definition based on the governing board’s determination that such a definition is appropriate for their target population and service area. As with all sliding fee discount program policies, the health center’s family size definition must be applied uniformly to all patients.
8) What steps must a health center take if an individual who is auto-assigned to another Medicaid managed care provider wishes to be a health center patient?
The health center would inform/educate individuals regarding their option to receive care from their assigned primary care provider. In cases where the individual requests to be re-assigned to the health center, the health center may also provide assistance with the process of reassignment/re-enrollment consistent with health center policies and procedures and any additional guidance provided by the state
Medicaid agency or state law. Once registered by the health center, such individuals must be assessed for income and family size in accordance with health center policies and procedures, and charged based on the health center’s SFDS, if applicable.
9) How would a health center count the number of pay classes in the sliding fee discount scale for the purpose of determining if the SFDS meets the “3 or more” pay classes rule?
The health center should count the number of pay classes above 100 percent and at or below 200 percent of the Federal Poverty Guidelines.
For example, in the following sample SFDS, the sliding fee discount schedule has four pay classes (B, C, D, and E) above 100% of the FPG and at or below 200% of the FPG.
Class A: 100% and below of the FPG
Class B: 101% – 125% of the FPG
Class C: 126% – 150% of the FPG
Class D: 151% – 175% of the FPG
Class E: 176% – 200% of the FPG
Class F: Above 200% of the FPG
All health center SFDSs must have at least three discount pay classes above 100 percent and at or below 200 percent of the Federal Poverty Guidelines.
10) Are health centers required to have a nominal charge for individuals at or below 100% FPG?
No. The decision to have a nominal charge is at the discretion of the health center governing board.
11) What is considered a nominal charge?
A nominal charge must be a fixed fee that does not reflect the true value of the service(s) provided and is considered nominal from the perspective of the patient. In addition, it is not intended to create a payment threshold for patients to receive care. Nominal charges are not “minimum fees,” “minimum charges,” or “co-pays.” Health center boards are responsible for determining whether the establishment of a nominal charge is appropriate for the target population. If electing to do so, the board must set a nominal charge(s) that meets the definition above. As with all sliding fee discount program policies, the health center’s nominal charge(s) must be applied uniformly to all patients.
Health centers may NOT require patients to enroll in public or private insurance and/or related third party coverage
12) Is it permissible for health centers to require proof of application/proof of denial for insurance or other documentation (e.g., exemptions) before offering services on a sliding fee discount schedule (SFDS)?
No. Health centers may not require patients to enroll in public or private insurance and/or related third party coverage, nor may eligibility for sliding fee discounts be based on factors other than income and family size. If a current or new patient is not able to, is exempt from, or chooses not to pursue insurance coverage, the health center must continue to serve that patient, and charge the patient in accordance
with the health center’s SFDS for the service(s) provided, as applicable. As a reminder, health centers must educate patients on options available to them based on their eligibility for insurance and/or related third party coverage.
13) Are insured patients who are at or below 200% of the Federal Poverty Guidelines eligible for the sliding fee discount program?
Yes, subject to the potential legal and contractual limitations. Please see Pages 11-12 of PIN 2014-02 for
an example.
14) In order to reduce barriers to care and improve health outcomes, a health center wants to purchase eyeglasses from a third party for its patients who receive optometry services. Although eyeglasses are related to optometry services, they are not typically included in the
optometry service based on prevailing standards of care. If the locally prevailing charge for eyeglasses is $100 and the total cost to the health center is $30, may we charge patients a flat fee of $40?
Yes. This type of supply/material (eyeglasses) falls within the category described in Section VII.F: Sliding Fee Discount Schedule: Other Considerations. As long as the health center has determined that the charge for this supply is less than the locally prevailing charge and this below-market charge facilitates patient access to this supply, this structure for charging the patient is permissible. Any revenue generated from these charges must be used to further the objectives of the project by benefiting the health center’s patient/target population, and for purposes not specifically prohibited under section 330.
PIN Section VIII. Billing and Collections
15) Are health centers required to participate in all insurance plans?
No. Health centers are required to participate in Medicaid and CHIP and must make every reasonable effort to collect reimbursement from Medicare, Medicaid, CHIP, and other private and public third party payors in order to maximize revenue from these sources. Beyond these requirements, health centers should consider their target population(s) and the costs and benefits of such participation when determining the specific public and private health insurance plans in which to participate (e.g., Medicaid managed care plans, Qualified Health Plans).
Sliding Fee Discount and Related Billing and Collections Program Requirements:
Frequently Asked Questions (FAQs)
NOTE: New FAQs will be added as necessary. For questions regarding Outreach and Enrollment, please see the Outreach and Enrollment page: http://bphc.hrsa.gov/outreachandenrollment/index.html
PIN Section II: Applicability
1) My health center receives Section 330(h) funds. Do I have to follow the requirements of the PIN for my homeless patient population?
Yes. This PIN applies to all health centers funded under the Health Center Program authorized in section 330 of the Public Health Service Act, as amended. The PIN also applies to look-alikes, as they must meet the statutory, regulatory and policy requirements for health center program grantees under section 330. While all health centers must uniformly apply the requirements clarified in the PIN to their patient
populations, HRSA recognizes the unique challenges of serving special populations and emphasizes that a health center must consider the characteristics of its overall patient population and that population’s barriers to care when establishing and evaluating their sliding fee discount programs.
PIN Section V. Governing Board Oversight
2) Does my governing board need to develop and approve the supporting sliding fee discount program operating procedures?
No. Governing boards are required to approve the sliding fee discount program policies that establish the foundation for operating procedures. Development and implementation of related supporting operating procedures rests with the health center staff under the direction of the key management staff.
PIN Section VI: Fee Schedule
3) Are health centers permitted to have a single line on their fee schedule for a “diabetes visit” that includes the provider encounter, lab work, and a mini-session with our nutritionist?
Yes. When constructing the fee schedule, a specific health center service along with associated laboratory services and/or medically related supplies and equipment may be combined into a single fee, as long as this is consistent with both prevailing standards of care and locally prevailing charges. See Section VI.A: Fee Schedule: Services for more detail.
PIN Section VII: Sliding Fee Discount Schedule
4) Do health centers have to assess income and family size for all patients including insured patients?
Health centers must assess income and family size for all patients, both for Health Center Program reporting purposes (See UDS Reporting manual) and for determining whether they are eligible for sliding fee discounts. Eligibility for sliding fee discounts is based on income and family size and no other factors.
Health Centers May NOT Use Assets Tests as Additional Eligibility Threshold
5) Is it permissible for a health center to include assets in its definition of income?
No. Health centers may not use assets tests as an additional eligibility threshold, nor may they create a “net worth test” (i.e., a combined threshold of assets and income). Assets are not considered income; assets are an economic resource, while income is comprised of earnings over a given period of time. For example, a rental property would be considered an “asset,” but the income generated from this rental
property could be considered “income.” Health centers are permitted to request information on assets for purposes other than sliding fee discount scale eligibility, e.g., assessing eligibility for private or public benefit programs that require asset information.
6) What does a health center have to include in assessing and documenting a patient’s income?
The health center governing board determines in policy what types of income are included or excluded in defining “income,” as well as the associated documentation needed to assess income for individual patients, as long as such policies do not create barriers to care. As with all sliding fee discount program policies, the health center’s nominal charge(s) must be applied uniformly to all patients.
7) How do health centers consider family members, not living with the patient but largely supported by the patient’s income, in their definition of “family size”?
Health centers have the flexibility to define family size to include these family members as part of their definition based on the governing board’s determination that such a definition is appropriate for their target population and service area. As with all sliding fee discount program policies, the health center’s family size definition must be applied uniformly to all patients.
8) What steps must a health center take if an individual who is auto-assigned to another Medicaid managed care provider wishes to be a health center patient?
The health center would inform/educate individuals regarding their option to receive care from their assigned primary care provider. In cases where the individual requests to be re-assigned to the health center, the health center may also provide assistance with the process of reassignment/re-enrollment consistent with health center policies and procedures and any additional guidance provided by the state
Medicaid agency or state law. Once registered by the health center, such individuals must be assessed for income and family size in accordance with health center policies and procedures, and charged based on the health center’s SFDS, if applicable.
9) How would a health center count the number of pay classes in the sliding fee discount scale for the purpose of determining if the SFDS meets the “3 or more” pay classes rule?
The health center should count the number of pay classes above 100 percent and at or below 200 percent of the Federal Poverty Guidelines.
For example, in the following sample SFDS, the sliding fee discount schedule has four pay classes (B, C, D, and E) above 100% of the FPG and at or below 200% of the FPG.
Class A: 100% and below of the FPG
Class B: 101% – 125% of the FPG
Class C: 126% – 150% of the FPG
Class D: 151% – 175% of the FPG
Class E: 176% – 200% of the FPG
Class F: Above 200% of the FPG
All health center SFDSs must have at least three discount pay classes above 100 percent and at or below 200 percent of the Federal Poverty Guidelines.
10) Are health centers required to have a nominal charge for individuals at or below 100% FPG?
No. The decision to have a nominal charge is at the discretion of the health center governing board.
11) What is considered a nominal charge?
A nominal charge must be a fixed fee that does not reflect the true value of the service(s) provided and is considered nominal from the perspective of the patient. In addition, it is not intended to create a payment threshold for patients to receive care. Nominal charges are not “minimum fees,” “minimum charges,” or “co-pays.” Health center boards are responsible for determining whether the establishment of a nominal charge is appropriate for the target population. If electing to do so, the board must set a nominal charge(s) that meets the definition above. As with all sliding fee discount program policies, the health center’s nominal charge(s) must be applied uniformly to all patients.
Health centers may NOT require patients to enroll in public or private insurance and/or related third party coverage
12) Is it permissible for health centers to require proof of application/proof of denial for insurance or other documentation (e.g., exemptions) before offering services on a sliding fee discount schedule (SFDS)?
No. Health centers may not require patients to enroll in public or private insurance and/or related third party coverage, nor may eligibility for sliding fee discounts be based on factors other than income and family size. If a current or new patient is not able to, is exempt from, or chooses not to pursue insurance coverage, the health center must continue to serve that patient, and charge the patient in accordance
with the health center’s SFDS for the service(s) provided, as applicable. As a reminder, health centers must educate patients on options available to them based on their eligibility for insurance and/or related third party coverage.
13) Are insured patients who are at or below 200% of the Federal Poverty Guidelines eligible for the sliding fee discount program?
Yes, subject to the potential legal and contractual limitations. Please see Pages 11-12 of PIN 2014-02 for
an example.
14) In order to reduce barriers to care and improve health outcomes, a health center wants to purchase eyeglasses from a third party for its patients who receive optometry services. Although eyeglasses are related to optometry services, they are not typically included in the
optometry service based on prevailing standards of care. If the locally prevailing charge for eyeglasses is $100 and the total cost to the health center is $30, may we charge patients a flat fee of $40?
Yes. This type of supply/material (eyeglasses) falls within the category described in Section VII.F: Sliding Fee Discount Schedule: Other Considerations. As long as the health center has determined that the charge for this supply is less than the locally prevailing charge and this below-market charge facilitates patient access to this supply, this structure for charging the patient is permissible. Any revenue generated from these charges must be used to further the objectives of the project by benefiting the health center’s patient/target population, and for purposes not specifically prohibited under section 330.
PIN Section VIII. Billing and Collections
15) Are health centers required to participate in all insurance plans?
No. Health centers are required to participate in Medicaid and CHIP and must make every reasonable effort to collect reimbursement from Medicare, Medicaid, CHIP, and other private and public third party payors in order to maximize revenue from these sources. Beyond these requirements, health centers should consider their target population(s) and the costs and benefits of such participation when determining the specific public and private health insurance plans in which to participate (e.g., Medicaid managed care plans, Qualified Health Plans).